|
In general, immuocompetent humans have a high level of innate immunity to fungi and most of the infections they cause are mild and self-limiting. This resistance is due to:
When fungi do pass the resistance barriers of the human body and establish infections, the infections are classified according to the tissue levels initially colonized . This is often experienced in the hospital setting although underreported in the USA. Recent studies in France indicate nearly half of the nosocomial infections (hospital acquired infections) of Aspergillosis result in death even when the surgery is successful by this fungal mold. More commonly the clinician will encounter fungal mold infections as a topical presentation such as in the case of the common dermatophytes typically in the scalp and nails.
Classes of Mold Infection (Dermatophytes) at Tissue Level A. Superficial mycoses - infections
limited to the outermost layers of the skin and hair. The superficial
mycoses are: B. Cutaneous mycoses - infections that extend deeper into the epidermis, as well as invasive hair and nail diseases. These diseases are restricted
to the keratinized layers of the skin, hair and nails. Unlike the superficial
mycoses, various cellular immune responses may be evoked, causing pathologic
changes in the host that may be expressed in the deeper layers of the
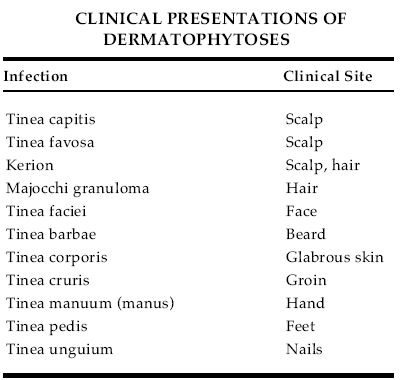
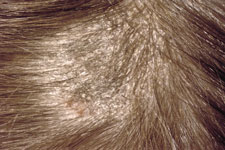
skin. The agents causing these diseases are termed dermatophytes. The
diseases are referred to as ringworm or tinea. All of the dermatophytic diseases are
caused by members of three genera, Microsporum, Trichophyton and Epidermophyton, which comprise 41 species. The cutaneous
mycoses are:
C. Subcutaneous mycoses - infections involving the dermis, subcutaneous tissues, muscle and fascia These infections initially
involve the deeper layers of the dermis, subcutaneous tissue or bone.
Most infections have a chronic or insidious growth pattern, eventually extending into the epidermis
and are expressed clinically as lesions on the skin surface. They are initiated by trauma to the skin and
are difficult to treat and surgical intervention (excision or amputation) is frequently employed. The subcutaneous mycoses are:
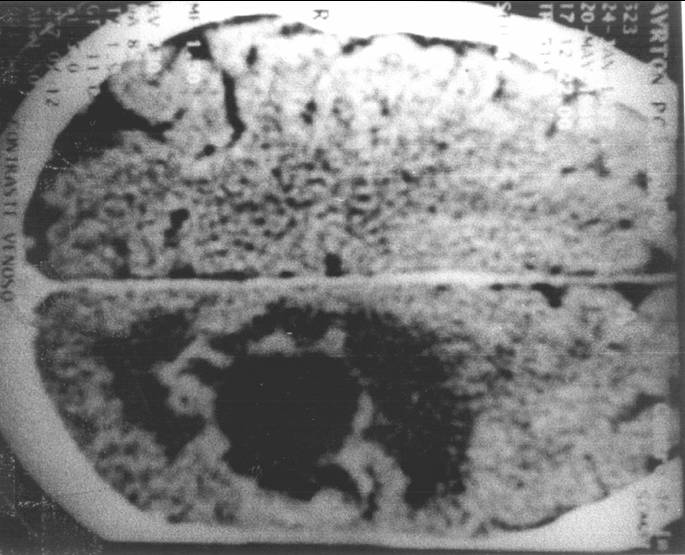
D. Systemic Mycoses - Infections that originate primarily in the lung (RECENT CASE: Aspergillus niger Fungal ball- Kendall Park, NJ 2004) and may spread to many organ systems, eye, intestines, spine, heart (endocarditis, pericarditis ) brain, kidney etc.
Aspergillus in the Lung We investigated a habitation in 2006 in Monmouth County, New Jersey. A 65 year male initially diagnosed with a brain cancer, then as Aspergillosis. . Lab culture analysis revealed Cladophialophora (Xylohypha) bantiana. This pathogen was found extensively in the damp basement.
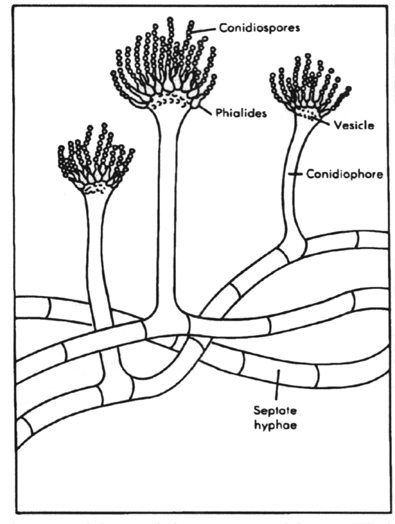
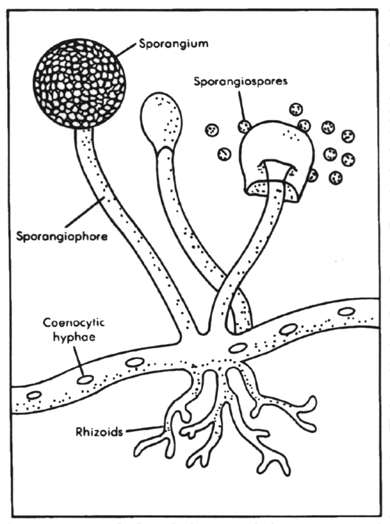
Unlike most other fungi, the five systemic mycotic agents are inherently virulent. Each species has biochemical and structural features that enable it to evade host defenses. The primary focus of infection is the lung but secondary infection may occur elsewhere in the body. The five etiological agents are identified by their morphology on agar plates (saprobic phase) and in tissue (parasitic phase): Dimorphic with mold to yeast transition when infecting susceptible species. Yeast cells are relatively small. Saprobic phase shows tuberculate macroconidia. 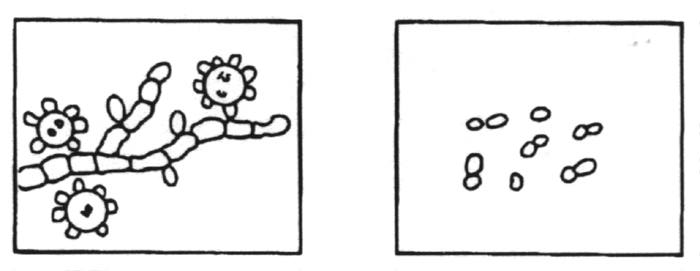
Saprobic Phase Parasitic Phase Dimorphic with mold to yeast transition when infecting susceptible species. Yeast cells are medium size with thick walls. 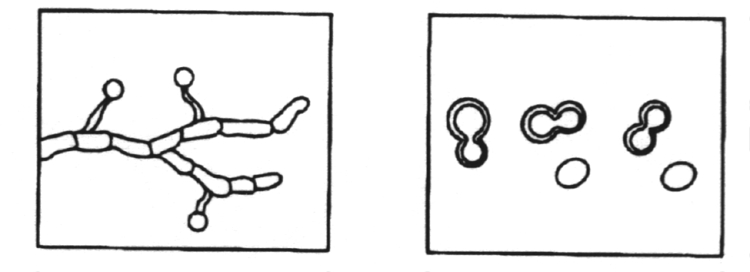
Saprobic Phase Parasitic Phase Dimorphic with mold to yeast transition when infecting susceptible species. Yeast cells have multiple buds. 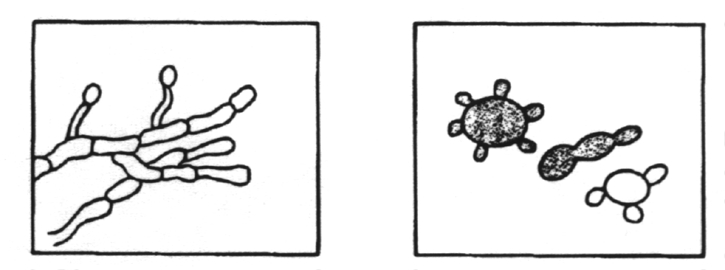
Saprobic Phase Parasitic Phase Dimorphic with mold to spherule transition when infecting susceptible species. Spherules are multinucleate. 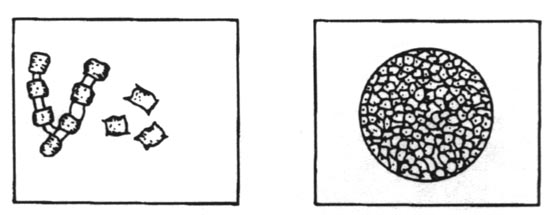
Saprobic Phase Parasitic Phase Monomorphic with yeast phase only. This is the only pathogenic yeast with a capsule. The capsule is extremely large. 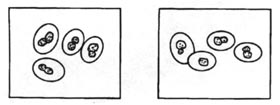
Saprobic Phase Parasitic Phase E. Opportunistic mycoses - infections in patients with immune deficiencies who would otherwise not be infected Opportunistic mycoses
are seen in those people with impaired host defenses such as occurs
in The major opportunistic
mycoses include:
F. Bronchial Asthma
- Fungal mold appears to be a leading cause of asthma and certainly
plays a role in aggravating asthmatic conditions as demonstrated
in recent studies where IgE
is clearly elevated when
contact is made with mold in a 2004 study.
F. Sarcoidosis (or sarcoid) is an immune system disorder characterized by non-necrotising granulomas (small inflammatory nodules). Virtually any organ can be affected, however, granulomas most often appear in the lungs (D860) or the lymph nodes (D861). Symptoms can occasionally appear suddenly but more often than not appear gradually. When viewing X-rays of the lungs, sarcoidosis can have the appearance of tuberculosis or lymphoma. Antifungal AgentsAmphotericin B - Polyene Antibiotics (macrolides)Amphotericin B - binds to ergosterol moiety in the plasma membrane causing derangement of the membrane integrity and leakage of cytoplasmic contents. Administered systemically. 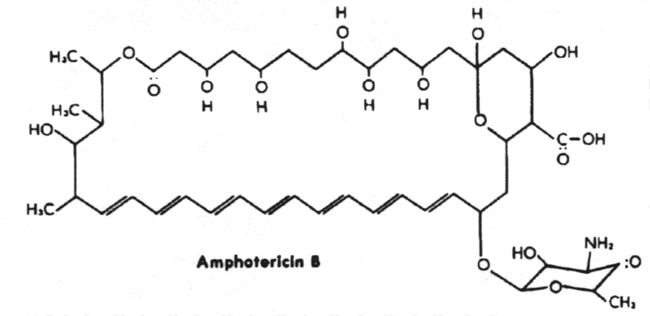
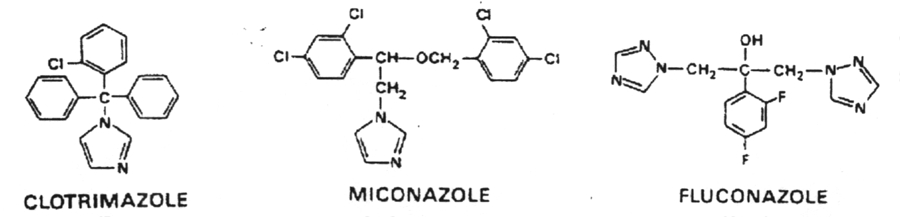
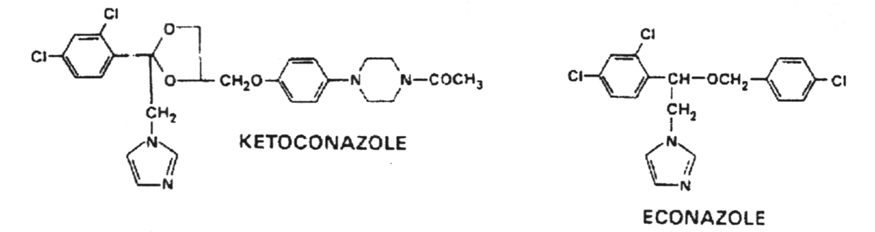
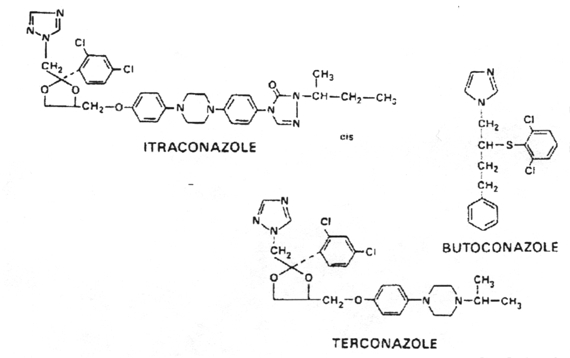
Nystatin - binds to ergosterol and disrupts plasma membrane. Highly insoluble and toxic and therefore used topically only. AzolesBlock ergosterol synthesis at one or more sites
with the accumulation of 14 -methyl sterol (which replaces ergosterol
in the plasma membrane causing selective leakage and increased osmotic
sensitivity). They also disrupt chitin synthesis. All effects are
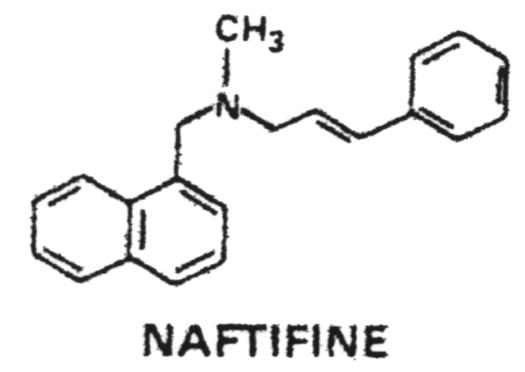
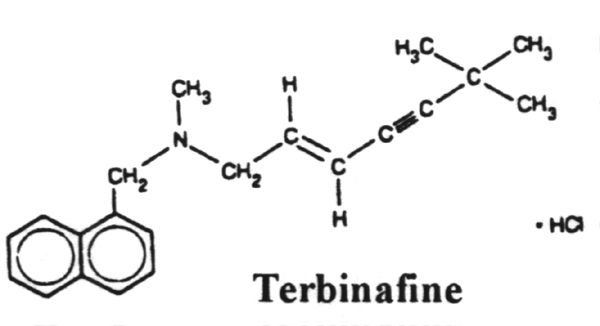
due to the binding to cytochrome P-450. Allylamines
Echinocandins Echinocandins are a new option for fungal infections. They are fungicidal and less toxic to the host by virtue of their novel mechanism of action. They are b-1, 3-glucan synthase inhibitors. FDA, USA has approved caspofungin for treatment of invasive aspergillosis in patients who fail to respond or are unable to tolerate other antifungals. Two other agents are in phase III clinical trials – micafungin and anidulafungin. Caspofungin among echinocandins has been studied vastly and offers apparent exciting advantages of a broad spectrum of activity including strains of fungi resistant to other antifungal agents, tolerability profile, with no nephrotoxicity and hepatotoxicity as compared to azole and macrolide antifungals. It may be effective in AIDS-related candidal esophagitis, oropharyngeal candidiasis, fungal pneumonia and nonmeningeal coccidioidomycosis. Clinical trials are required to ascertain their safety in special groups—pediatric, pregnant and nursing mothers. Echinocandins provide an exciting option for combination therapy with other antifungals in fulminant fungal infections.
Pyrimidine analogs 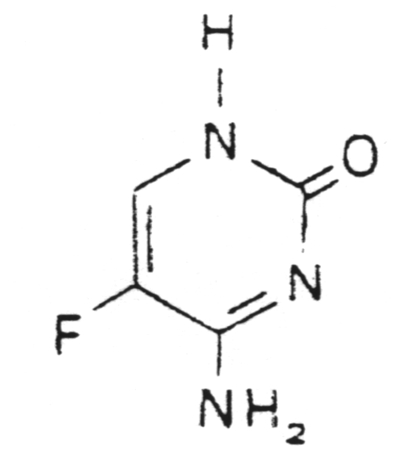
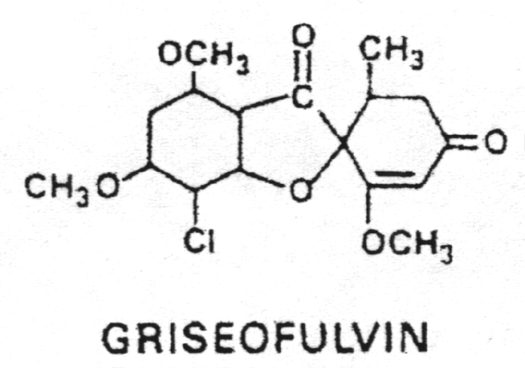
Miscellaneous types
Potassium iodide (KI) - Given orally for sporotrichosis 5. Diagnosis of mold illness and fungal diseases We refer you to Dr. Ritche Shoemaker's Diagnostic Protocol for Mold Related Illness 1. Morphologically
fungi are unicellular (yeasts) or multicellular (hyphae). Some fungi
can alternate between the two forms 3. Hyphae reproduce asexually via the formation of spores termed microconidia or macroconidia. 4. Fungi produce toxins such as ergot alkaloids, psychotropic agents and aflatoxins. 5. Visualization
of fungi in human tissue is accomplished by treatment with 10% KOH
and staining with lactophenol cotton blue, 6. India ink may be used as a negative stain to emphasize the capsule of yeast. 7. The
physician can use an ultraviolet lamp (Wood's lamp) to detect fluorescent
compounds produced by fungi growing in or on 8. Fungal
diseases are classified according to their depth of penetration of
human tissue. Thus, there are the superficial mycoses,
9. The superficial mycoses include pityriasis versicolor, tinea nigra, black piedra and white piedra. 10. The cutaneous mycoses (tineas or ringworms) are restricted to growth in the keratinized layers of the skin, hair and nails. 11. The
subcutaneous mycoses penetrate the dermis, subcutaneous tissue, muscle
and fascia. These include sporotrichosis, 12. Systemic
mycoses originate in the lung and then may spread to many organ systems.
These include histoplasmosis, North 13. Fungi are most commonly cultured on Sabouraud's agar or Mycosel agar. 14. Opportunistic
mycoses are often secondary to other diseases that compromise host
immunity such as AIDS, diabetes, and 15. Antifungal
agents are classified according to their chemical structure as macrolides,
azoles, allylamines, pyrimidine analogs 16. The polyene antifungals are amphotericin B and nystatin which bind to ergosterol in the plasma membrane, thus disrupting it. 17. The
azole antifungals include fluconazole and ketoconazole plus numerous
others. They all block ergosterol synthesis by 18. The allylamines include naftifine and terbinafine which inhibit squalene epoxidase, thus blocking ergosterol synthesis. 19. The
pyrimidine analogs such as flucytosine incorporate into RNA and/or
DNA thus blocking protein synthesis or DNA 20. The miscellaneous antifungals include griseofulvin, haloprogin, ciclopirox olamine, tolnaftate and potassium iodide. 21. The three genera of dermatophytes are Microsporum, Trichophyton and Epidermophyton. |